
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Morton D, Pliske J, Renger F* and Luliak M
Corresponding Author: Fabian Renger, St. Elisabeth-University of Health and Social Work Bratislava, Slovakia, Germany.
Received: January 15, 2025 ; Revised: January 26, 2025 ; Accepted: January 29, 2025 ; Available Online: February 17, 2025
Citation: Morton D, Pliske J, Renger F & Luliak M. (2025) Spinal Manipulation Increases Maximum Voluntary Contraction and Cortical Drive: A Narrative Review. J Nurs Midwifery Res, 4(1): 1-8.
Copyrights: ©2025 Morton D, Pliske J, Renger F & Luliak M. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Objective: The broad purpose of this review is to display and synthesize works to date that unfold if changes in cortical output are an asset of chiropractic care, leading to increased muscle function. Findings in this field support an extensive yet realistic model of understanding spinal manipulation, which, if further researched, can help to develop new strategies of therapy, prevention, and performance in different fields.
Methods: From October 2022 to February 2023, the Dimensions and PubMed electronic database was researched for relevant trials occurring from 2010 to 2022. Inclusion criteria covered publication in peer-reviewed journals and the application of manual HVLA manipulation as the intervention. Study designs were created or adopted mainly to research cortical function on neurologically healthy individuals.
Results: Subjects presented considerably increased corticospinal activity and maximum strength directly post intervention for the relatively short observational time frame. Primarily, transcranial magnetic stimulation (TMS) and electromyography (EMG) had been used sufficiently for assessment.
Conclusion: Neuromuscular effects of spinal manipulation occur frequently. Further research is necessary and indicated in order to make these facts accessible to the public in a practical and meaningful way.
Research Question: Do HVLA manipulations have a conductive impact on cortical drive?
Keywords: Spinal manipulation, Chiropractic, HVLA manipulation, Cortical drive, Brain function, Joint manipulation
INTRODUCTION
Over the past few decades, the chiropractic profession has been seen as a low-cost treatment for back and neck pain. Multiple studies have shown positive outcomes in this field [1]. A growing body of evidence displays several measurable effects of chiropractic care, that are unexpected at first sight but potentially most valuable in preventive healthcare as well as in other fields. These modifiable parameters among others are balance, flexibility, endurance, and even improvements in cognitive function [2,3]. The traditional frame that chiropractic professionals use to explain these phenomena has been the so-called bone out of place, or “subluxation” model; an idea that describes misaligned vertebrae in the spinal column and how they irritate spinal nerves in such a way that most basic bodily functions suffer a decrease in efficiency. Consequently, the goal of chiropractic was to reverse this process and restore function. While this model has been used to explain any non-orthopedic effect of chiropractic care, from a scientific perspective, it is problematic since it is hardly compatible with the current knowledge of anatomy and neurophysiology [4]. Recent years have brought forward a new field of chiropractic research that focuses mainly on the direct impact spinal manipulation has on brain function. Relating closely to the concepts of functional neurology, the spine is seen as an integrative structure, which, by having high-velocity low-amplitude (HVLA) manipulation applied to it, generates sensory and motor activity in certain areas of the brain that has therapeutic or even neuroplastic effects [5]. This brain-stimulative model of chiropractic is more consistent with physiology and therefore a more likely explanation for the various beneficial apparitions that have been documented by chiropractors over recent decades. One of the factors presented to be highly reactive is muscle strength. An example has been observed in an award-winning paper from 2011, when improvements in grip force of up to 16.82% in elite judo athletes occurred directly following chiropractic intervention [6]. There is a tendency in literature to understand phenomena like these as a side effect of decreasing symptoms [7,8], but ongoing research shows an effect of HVLA manipulation on sensorimotor integration that seems applicable to many different populations, eventually having therapeutic, preventive, or optimizing characteristics [9]. Cortical output and the extent of motor unit recruitment are a relatively straight connection on the neuroaxis that correlates with strength improvements [10]. Directly displaying neuro-excitatory properties of spinal manipulation via this actuality seems plausible and, if understood and cultivated properly, can potentially be of value in many fields, such as neurology, rehab, or even sports. Therefore, the broad purpose of this review is to summarize research to date that highlights changes in cortical drive as a possible asset of chiropractic treatment.
CORTICAL DRIVE
The most basic understanding of neuronal operation is the “integrate and fire” model, in which neurons integrate synaptic activity until a threshold is reached and accordingly an action potential is generated [11]. More recently, the literature has delivered a more complex understanding of neurons, their firing patterns, and the ways they interact. While gas exchange and nutritional supply play a key role in neuron integrity, adequate and sufficient stimulation in the form of constant electrical and chemical exchange is a third and essential component of leaving neurons in an optimal central integrative state (CIS) [12]. Parts of the electrochemical energy required to support neuron function emerge from receptor response to environmental signals. It is therefore necessary that receptors undergo activation to fuel the neuron pools they are connected to. All systems, including those that are not constantly active-for example, optical radiations or cortical cells involved in memory-need constant stimulation to maintain a healthy CIS. It is supplied to the neuroaxis by constant stimulus pathways that integrate the detection of motion or the effects of gravity, enabling the brain’s vital functions, such as building up ATP and proteins. A major part of constant pathway receptors is localized in the axial weight-bearing structures such as the muscles, ligaments, and joints of the spine and ribs. By providing subthreshold activation (excitation), these systems compensate for the periods of inactivity of nonconstant systems [13]. A practical example underlining the various integrations of spinal pathways is the presentation of how upper-cervical manipulation has an influence on physical blind-spot size. In principle, stimulation of weight bearing structures has an excitatory influence on many functional units of the brain [14]. Excitation brings a neuron`s membrane potential closer to threshold, based on the energy it receives. The excited state supports supply and the probability of generating an action potential is increased. Consequently, stimulation causes more intense activation of neuron pools or whole functional brain areas [15,13]. Afferences from triggered spinal receptors and muscle spindles run to the ipsilateral cerebellum via the spinocerebellar tract and reach the contralateral cortex via cerebellorubral and rubrothalamic tracts, acting excitatory. The prefrontal cortex has shown to be highly reactive to accelerated stimulation of this pathway system [16]. Therefore, it is plausible that receptor activation of the spine via HVLA manipulation produces changes in cortical excitability leading to stronger central commands, referred to as “cortical drive,” which alter the extent of motoric functions.
HVLA MANIPULATION
Manually applied HVLA techniques are a common approach in the field of chiropractic. Although it can be done to nearly every joint of the human body, chiropractors typically (but not exclusively) manipulate or “adjust” (as intern terminology has it) segments of the spinal column. As mentioned above, recent literature has revealed that the spine is not just interesting for its tendency to cause pain syndromes but also for its complex network of receptors and pathways integrating into multiple brain regions [17]. Spinal dysfunction is commonly defined as a multifactorial, self-perpetuating phenomenon involving joint motion and the brain’s ability to effect sensory integration and the production of proper motor output [18]. By making an adjustment, the chiropractor aims to restore the natural coupled motion patterns and thus generate related brain activity. Before application, the spine is palpated for indicators of disfunction, such as tenderness, abnormal or restricted joint play, asymmetric intervertebral muscle tension, or a lack of range of motion. Also, the patient history and the degenerative status of the spine are taken into consideration. After the involved joints are identified, they are brought to a point of tension and an HVLA thrust is delivered [19]. Successful manual manipulation is mostly, but not necessarily, accompanied by an audible release. Herzog [20] were able to demonstrate that the speed of force application is a key factor for evoking the full spectrum of effects, which is important for this review. As mentioned, spinal manipulation produces significant neuronal responses that indicate an impact on cortical function, provided that the thrust is applied in a time frame of 200-400ms. It has been shown that even if an audible response was elicited, insufficient velocity does not lead to the desired patterns [20]. Therefore, clinicians must be skilled in practice and well selected for research activities.
METHOD
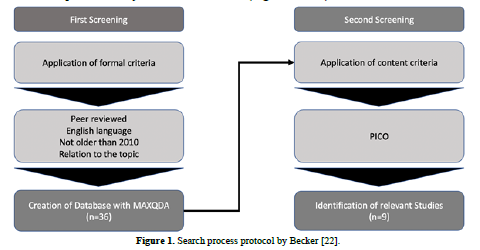
The method for conducting this research was a systematic selection process performed from October 2022 until February 2023 [21]. The Dimensions and PubMed database was researched for the relevant literature. The search was limited to articles in English. Search terms were “chiropractic,” “spinal manipulation,” “spinal adjustment,” and “chiro” in combination (AND) with “cortical drive,” “muscle strength,” and “brain.” In addition, manual searches based on reference lists in identified articles were performed to complete the process.
Research question: Do HVLA manipulations have a conductive impact on cortical drive?
ELIGIBILITY
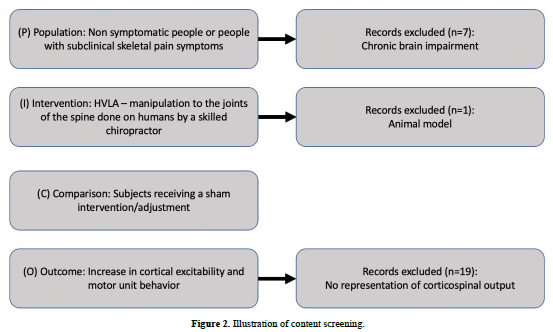
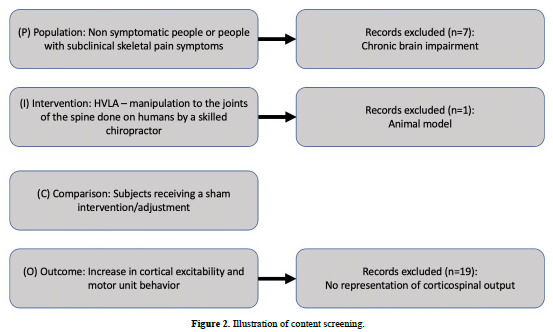
Trials conducted no earlier than 2010 and which underwent a peer-review process were further examined. To make sure that improvements occurred on the cortical level of the neuroaxis, only trials that proceeded by implementing a technology or diagnostic process that allowed for conclusions about corticospinal activity were included. Extensive reactions to the intervention had to be possible, so trials were excluded that focused on stroke patients, as well as those with any kind of permanent damage to the brain or a neurodegenerative disease. Chiropractic is a field that consists of different techniques and approaches. Manual manipulation has been researched for its requirements and impacts [20]. Therefore, approaches like tool-assisted chiropractic were not included. Also, any type of animal research on the topic has not been taken into consideration (Figures 1 & 2).
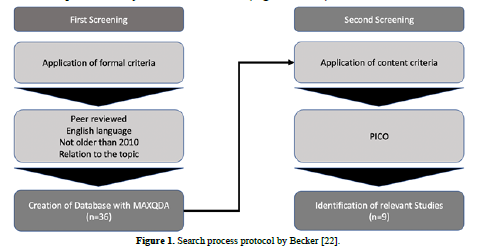
RESULTS
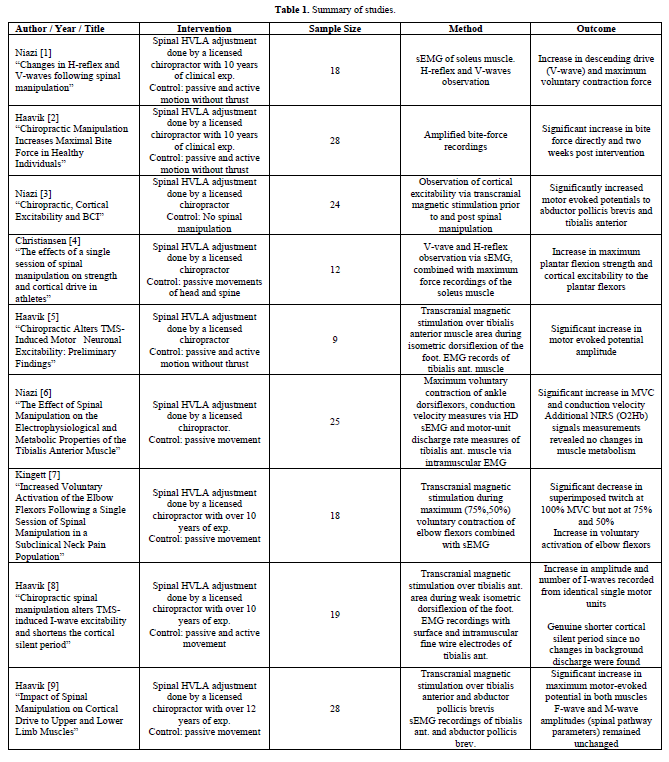
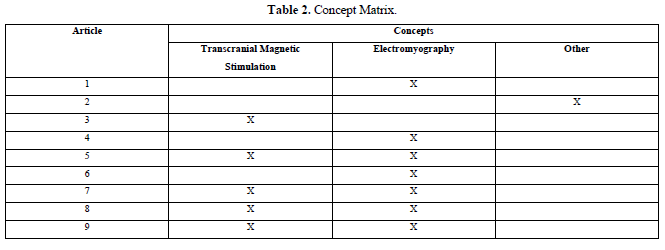
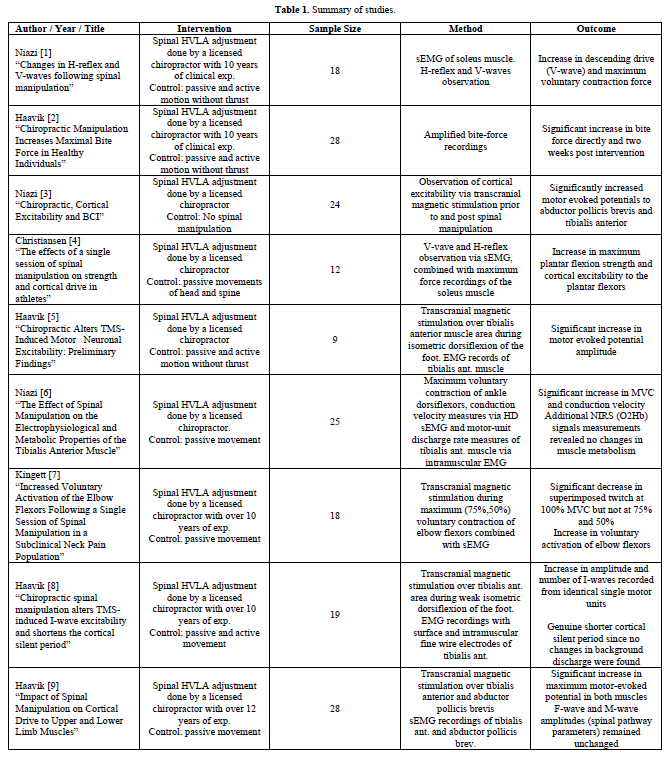
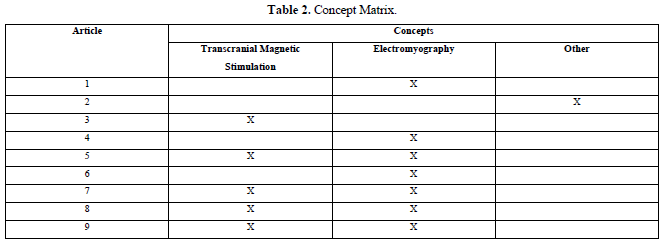
In the end, nine papers fulfilled the set criteria. The authors provided insights in cortical activity by specifically modified use of transcranial magnetic stimulation (TMS) and electromyography (EMG). One report featured bite force measurements, working on the hypothesis that central effects of care must be measurable in cranial nerve-innervated muscles (Tables 1 & 2).
DISCUSSION
We found insights that showed effects on maximum voluntary contraction (MVC) and strength, as well as cortical drive. HVLA manipulation seems to generate an immediate effect in cortical areas that causes differences in output intensity by altering the balance between excitatory and inhibitory activity. This was displayed by the electromyographic and transcranial magnetic stimulation parameters. Nearly half of the studies favored a combined approach. Among control groups, no noteworthy changes occurred. Designs had been created or partially adopted to clarify that orthopedic and symptomatic factors are not necessarily responsible for the described outcomes but are possibly an effect of improved neuromuscular regulation. The authors explicitly stated that their efforts and use of technology were oriented toward observing brain function on the cortical level.
EMG is understood as a series of procedures to evaluate neuromuscular integrity via repetitive nerve stimulation while observing different electrical signals as well as electrical representations of reflexes. It can be done invasively, incorporating needle-type electrodes, or noninvasively by using surface electrodes. The choice of approach to use depends on the clinical question. Recruiting several electromyographic parameters, such as the H-reflex, F-wave or V-wave, allows for conclusions regarding central and/or peripheral neuronal function and performance [23]. F-wave observation has been performed by Haavik et al. in the named experiments. The F-wave emerges from peripheral nerve stimulation, such as Nn. medianus and ulnaris for the upper and Nn. tibialis and peronaeus for the lower extremity. Electrical stimuli descend to the muscle itself, but also ascend to the alpha motoneuron in the spinal cord, provoking it to discharge and produce activity in the connected muscle tissue once again. Using consistent stimuli intensity permits the assessment of motoneuron excitability on the spinal cord level, thus ruling out spinal motoneurons as the cause of the change. As stated by Haavik et al., a weakness in this process is the small portion of the neuron pool that is tested. Conclusively, F-wave measures are indicative but not proof of consistent spinal cord excitability [24]. The H-reflex is a monosynaptic reflex, triggered by electric stimulation. It can typically be observed in weaker stimuli strength, since supramaximal stimuli irritate not just proprioceptive but also motoric fibers, causing a collision of signals that erases the H-reflex pattern [23]. However, by initiating voluntary contraction while the H-reflex is eradicated by supramaximal stimulation, orthodromic action potentials collide with the antidromic potentials evoked by the electrodes. Consequently, a part of the reflex activity is then free to reach the muscle tissue and produce a reading, the V-wave. This parameter is said to be a reliable measure of efferent cortical activity and has been used for that purpose, qualifying the report for this review [25,26]. Transcranial magnetic stimulation has been used as a primary assessment to aim for brain activity during spinal manipulation. It is a noninvasive method of directly observing cortical activity. Its use delivers insights into the extent of activation, localization, and resonance to stimuli to determine integrity and function of areas of the primary motor cortex. The procedure involves an electric pulse generator connected to a magnetic coil. Changing electric current within the coil generates a magnetic field that induces excitation of isolated neuron pools. The observation of the latter allows for various diagnostic conclusions or can be therapeutic [27]. In the listed chiropractic experiments, transcranial magnetic stimulation was mainly used to show changes in cortical excitability by displaying maximum motor-evoked potentials or the superimposed twitch amplitudes, before and after intervention [28,29]. It demonstrated good to moderate test–retest reliability for measures of motor cortex organization and excitability. Muscle representation areas remained relatively stable. Also, the motor threshold was assessed without noteworthy changes. Depending on the experimental goal, it is commonly used in combination with EMG settings to reach very specific amounts of muscle contraction while reading cortical activity. Even though there are differences in reliability, depending on the parameter, data confirms that observations via these technologies is a respectable approach that fits this setting. [30-32]. Improvements were shown in average people with or without subclinical symptoms, as well as in athletes. Other studies documented such observations in stroke patients or the elderly, indicating that chiropractic can be beneficial for a wide range of people, depending on the therapy goals [33,34]. However, these efforts were focused on immediate and short-term results. To determine if and how these effects can be long-lasting or permanent or can lead to beneficial neuroplastic changes, more treatment sessions and longer periods of observation time are required. A weakness, mentioned by the authors, is the difficulty researchers commonly face to establish a blinding procedure in experiments that involve manual therapy applications. The chiropractor will be aware whether his/her intervention is sufficient. Furthermore, chiropractic is a known approach, so we can assume that the subjects will realize any lack of the hoped-for effect. Efforts have been made to counteract this disappointment by choosing subjects who are naïve to chiropractic or by actively deceiving the control group [35]. But whether one can assume sufficient blinding by such tactics remains questionable. Yet, regarding the nature of the intervention and relative to the field of research, a good standard of quality was maintained in these studies. Although the sample sizes in the studies were quite small, the magnitude of several outcomes, compared to controls, seems unlikely to be exclusively due to the placebo effect.
CONCLUSION
Consistently, conductive changes of remarkable magnitude in cortical drive and strength have been found through chiropractic methods. The results deliver multiple imaginable uses when further researched. Firstly, the chiropractic profession has been seen as a subject closely related to orthopedics and physiotherapy. A huge problem is that some favorable results of this method cannot be explained reasonably using the traditional or orthopedic model, thus leading to speculation or even esoteric conclusions in the search for clarification. This causes issues regarding the identity and the role of chiropractors in modern healthcare [36,37]. Deeper knowledge of the mechanisms of action helps to understand surprisingly good or unsatisfactory results of the treatment, indications, and treatment plans and generally provides a foundation for efficient and successful application with a scientific background that chiropractors can be guided by. Secondly, a rapidly growing body of evidence-including this review-indicates that chiropractic care has direct effects on brain function, drawing a connection to the field of neurology. Initial cautious attempts to put that finding to therapeutic use have already been made and have raised hopes for complementary treatment or prevention strategies to support patients with neurological disorders, stroke, or neurodegenerative disease. Thirdly, muscle strength is one of five parameters of sports performance. Athletes already use chiropractic for injury prevention and as a musculoskeletal treatment. The knowledge summarized in this report, combined with the topics of other articles on chiropractic-for example, joint position sense or muscle coordination-can be interesting for sports sciences regarding performance optimization, as accentuated by Christiansen [26].
No Files Found




Internationally Accepted
Share Your Publication :